

Intravascular Lithotripsy (IVL): A Breakthrough in Treating Calcified Heart Arteries
Coronary artery disease (CAD) remains one of the leading causes of death worldwide. While stents and balloon angioplasty have revolutionized heart care, one major challenge persists: heavily calcified coronary arteries. When arteries are hardened by calcium deposits, stents may fail to expand fully, leading to poor outcomes.
To overcome this, cardiologists now use a cutting-edge technology called Intravascular Lithotripsy (IVL). Inspired by kidney stone treatment (extracorporeal shockwave lithotripsy), IVL uses sonic pressure waves to crack calcium inside blood vessels, making them easier to treat with stents.
What is Intravascular Lithotripsy (IVL)?
IVL is a minimally invasive technique performed during angioplasty to treat calcified coronary and peripheral arteries.
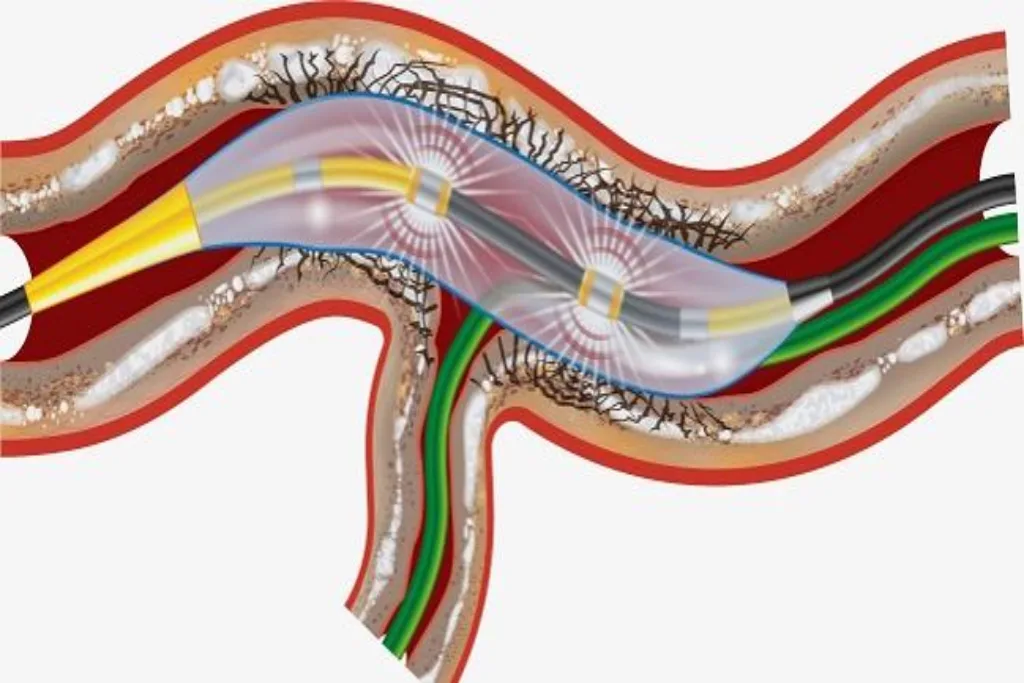
- It uses a special IVL balloon catheter equipped with emitters that generate acoustic (shockwave) pulses.
- These pulses travel through the fluid inside the balloon and selectively break up calcium within the arterial wall, while leaving soft tissues unharmed.
- Once the calcium is fractured, the artery becomes more compliant, allowing stents to expand properly.
Why is IVL Needed?
IVL is considered in cases where:
- The artery has severe, concentric, or nodular calcification.
- Balloons and stents cannot expand fully due to rigid calcium.
- Other techniques like Rotablation are unsuitable or risky.
- The patient has both coronary and peripheral artery disease.
Without plaque modification, deploying a stent in a calcified artery carries a high risk of under-expansion, restenosis, or stent fracture. IVL significantly reduces this risk.
How is IVL Performed? Step-by-Step
1. Patient Preparation
- IVL is performed in a cardiac cath lab under local anesthesia and mild sedation.
- Access is usually via the radial (wrist) artery or femoral (groin) artery.
- Continuous monitoring of ECG, oxygen levels, and blood pressure is done.
2. Arterial Access and Imaging
- A sheath is inserted into the access artery.
- A diagnostic catheter and guidewire are advanced to the coronary arteries.
- Angiography and sometimes intravascular imaging (IVUS or OCT) are performed to assess the extent of calcification.
3. Placement of the IVL Balloon
- A guidewire is passed across the calcified lesion.
- The IVL balloon catheter is positioned at the site of the blockage.
4. Lithotripsy (Calcium Cracking)
- The balloon is inflated at low pressure (around 4 atm) to make contact with the artery wall.
- The system delivers a series of acoustic shockwaves (usually 10 pulses at a time).
- Each pulse generates pressure waves that travel through the vessel wall, creating micro-fractures in both superficial and deep calcium.
- This process is repeated in cycles until the entire lesion is treated.
5. Balloon Angioplasty and Stent Placement
- After calcium modification, the balloon is further inflated to dilate the artery.
- A drug-eluting stent (DES) is placed to keep the artery open.
- Because the calcium has been cracked, the stent can expand uniformly and seat properly.
6. Final Checks
- A repeat angiogram is performed to confirm restored blood flow.
- The catheter is removed, and the access site is closed with pressure or a closure device.
The entire IVL procedure usually takes 45–90 minutes, depending on the complexity of the lesion.
What Happens to the Calcium After IVL?
Unlike Rotablation, IVL does not pulverize calcium into particles. Instead, it creates controlled fractures within the calcium itself, softening the vessel wall. The calcium stays in place but is no longer rigid, which allows the artery to expand when a stent is deployed.
Benefits of IVL
- Safe and Precise: Targets only calcium, sparing soft tissue.
- Effective for Deep Calcium: Works on both superficial and deep layers.
- Improved Stent Expansion: Reduces risk of stent under-expansion.
- Minimally Invasive: Performed via wrist or groin access.
- Versatile: Can be used in both coronary and peripheral arteries.
- Fewer Complications: Lower risk of artery perforation compared to some other plaque modification techniques.
Risks and Limitations
While IVL is considered safe, possible risks include:
- Vascular injury (rare).
- Transient heart rhythm changes during pulses.
- Bleeding or bruising at the catheter site.
- Rarely, vessel dissection or spasm.
Also, IVL may not be suitable for very small vessels or blockages with heavy thrombus (clot burden).


Recovery After IVL
- Most patients are discharged within 24 hours.
- Medications such as dual antiplatelet therapy (DAPT), statins, and heart medicines are continued.
- Normal activity can usually be resumed in a few days.
- Lifestyle changes (diet, exercise, quitting smoking) remain vital to prevent recurrence.
IVL vs. Rotablation: Key Difference
- Rotablation: Physically drills calcium into micro-particles with a diamond burr.
- IVL: Cracks calcium in place with sound waves.
- Both may be complementary, but IVL is considered gentler and safer in certain scenarios.
Conclusion
Intravascular Lithotripsy (IVL) is a revolutionary tool in interventional cardiology. By using acoustic shockwaves to fracture calcium inside arteries, it enables safer and more effective stent placement in patients with heavily calcified blockages.
If you have been diagnosed with calcified coronary artery disease, consult an experienced interventional cardiologist to see if IVL is the right treatment option. This advanced technology is helping more patients achieve better outcomes and a healthier future.